Printed from acutecaretesting.org
July 2010
Cardiac biomarkers for acute coronary syndrome and ongoing myocardial damage in heart failure





ACUTE CORONARY SYNDROME
Acute coronary syndrome (ACS) is characterized by abrupt plaque rupture and exposure of substances that promote platelet activation and thrombin generation. The resultant thrombus interruption of coronary blood flow results in myocardial necrosis.
An abrupt rupture or erosion of the vulnerable plaque with complete occlusion of blood flow by a so-called red thrombus results in ST-elevation myocardial infarction (STEMI). Less obstructive thrombi and those that are constituted by less robust fibrin formation and a greater proportion of platelets aggregates, so-called white thrombus, result in non-ST-elevation myocardial infarction (NSTEMI) (Fig. 1).
It is noticeable that the therapeutic algorithm does differ for these two different spectrums.
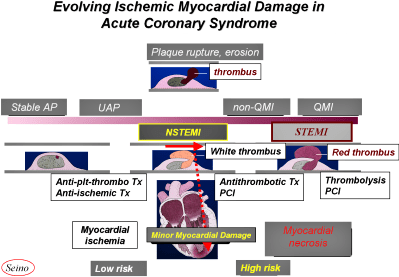
FIGURE 1: Evolving Ischemic Myocardial Damage in ACS - In case
of an abrupt rupture or erosion of such vulnerable plaque, complete
occlusion of blood flow by red thrombus results in STEMI, and less
obstructive thrombi and those that are constituted by less robust
fibrin formation and a greater proportion of platelets aggregates,
namely white thrombus produce NSTEMI. It is also noticeable that
the therapeutic algorithm does differ for the two
pathophysiologies.
CARDIAC BIOMARKERS FOR ACUTE CORONARY SYNDROME
The growing role of cardiac markers has been elucidated in patients with acute coronary syndrome, heart failure and other cardiovascular diseases.
The markers can be cytosolic like heart-type fatty-acid-binding protein (H-FABP) and creatine kinase MB (CKMB), myofibrillary like troponin T (TnT) and cardio-endocrine like B-type natriuretic peptide (BNP) and N-terminal proBNP (NT-proBNP) [1-5].
At present, these three groups of cardiac biomarkers are applied for detection of myocardial damage and the earlier diagnosis of acute coronary syndrome.
Our earlier investigation revealed that measurements of cardiac troponin T detected the presence of minor myocardial damage in patients with unstable angina, even when CKMB was not significantly elevated [1, 2], and those with minor myocardial damage showed higher risk for cardiac events (acute myocardial infarction, cardiac death, or necessity of emergency coronary revascularization) in the acute phase compared with those without minor myocardial damage [1-2].
In 2007, myocardial infarction was completely redefined based on clinical presentation, ECG findings and the elevation of cardiac troponin (using a troponin assay with an acceptable imprecision) instead of conventional CKMB measurements [6].
TROPONIN T AND H-FABP RAPID STRIP TEST FOR EARLIER DIAGNOSIS OF MYOCARDIAL INFARCTION
We developed a whole-blood rapid strip test for H-FABP and demonstrated the clinical utility for earlier diagnosis of myocardial infarction [3]. The diagnostic sensitivity and negative predictive value of the rapid H-FABP test were superior compared with those of a rapid TnT test, especially in the earlier-acute phase within 2 to 3 hour of onset of symptoms [3].
IMPORTANCE OF BNP OR NT-proBNP MEASUREMENT IN ACS
Large-scale clinical trials have demonstrated that BNP and NT-proBNP are increased in the early stage in acute coronary syndrome and can be used as powerful predictors of short- and long-term mortality. We have revealed different profiles of BNP (NT-proBNP) elevations between STEMI and NSTEMI [8].
The levels of conventional myocardial necrosis markers (CKMB and TnT) were on admission significantly higher in the STEMI group compared with the NSTEMI group [7]. However, conversely, NT-proBNP on admission was significantly higher in the NSTEMI group compared with the STEMI group, especially in the earlier phase.
When the correlation between TnT and NT-proBNP was analyzed and compared between STEMI and NSTEMI groups, the difference revealed augmented elevation of NT-proBNP in the NSTEMI group as compared with prominent elevation of TnT in the STEMI group, indicating development of larger ischemic insult despite of the smaller myocardial necrosis in NSTEMI compared with the STEMI group [7].
Data from FRISC trial [8] and also a substudy of PRISM [9] showed that NT-proBNP levels are highest on admission, within 24 hours of onset, decreased markedly the first 24 hours and then gradually over the following 6 months.
Interestingly, the predictive ability of NT-proBNP appears to increase with time, suggesting that persistent elevation is a particularly strong marker of adverse outcome. A second BNP or NT-proBNP value at 72 hours following the admission appeared to improve risk prediction concerning the end-point of death or recurrent MI at 30 days.
Regardless of the BNP or NT-proBNP value on admission, a NT-proBNP value > 250 pg/mL, or a BNP value > 80 pg/mL at 72 hours indicated a marked increased risk [8].
Although more data concerning the optimal timing of BNP or NT-proBNP measurements is warranted, it seems reasonable to measure BNP or NT-proBNP on presentation for initial fundamental risk assessment and once more during the sub-acute phase either at hospital discharge or at an early post-discharge outpatient visit for long-term risk assessment.
ONGOING MYOCARDIAL DAMAGE IN HEART FAILURE
Progressive deterioration of ventricular function is common in patients with severe chronic heart failure. We reported that detection of cardiac troponin T in blood identifies heart failure patients who are at increased risk of cardiac events [10].
Further, we have revealed that H-FABP, which is abundant in the cytosol of cardiomyocytes and, as described above, a sensitive marker of myocardial infarction, increased to a greater extent than TnT levels in heart failure patients who have ongoing myocardial damage [11].
Mean levels of H-FABP were greater in patients with NYHA class III or IV heart failure than in those with NYHA class II. Detection of TnT (≥ 0.02 ng/mL) was also more common in patients with worse heart failure (81 % in class III or IV vs. 43 % in class II (Fig. 2) [11].
Significant correlations were found between H-FABP levels and plasma levels of BNP and norepinephrine. Patients with ongoing myocardial damage (TnT ≥ 0.02 ng/mL or H-FABP ≥ 4.7 ng/mL) were independently associated with subsequent cardiac events (deaths or readmissions because of worsening heart failure) (Fig. 3) [11].
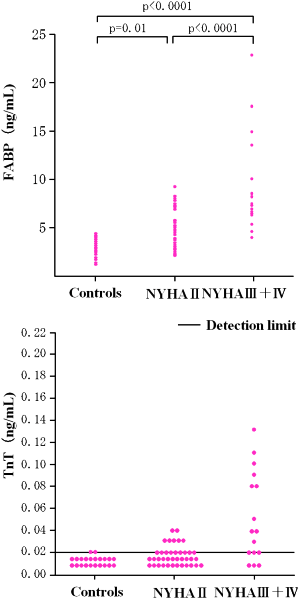
FIGURE 2: Detection of ongoing myocardial damage in chronic heart
failure by H-FABP and troponin T measurements.
Reproduced from Setsuta K, Seino Y, et al. Am J Med 2002; 113:
717-22 with permission from the publisher.
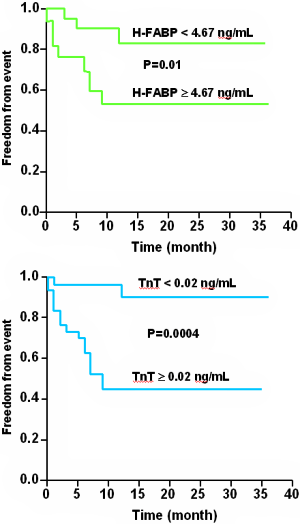
FIGURE 3: Prognostic value of H-FABP and troponin T
measurements in chronic heart failure.
Reproduced from Setsuta K, Seino Y, et al. Am J Med 2002; 113:
717-22 with permission from the publisher.
H-FABP and TnT are markers of ongoing myocardial damage and are associated with subsequent cardiac events in patients with chronic heart failure [10, 11].
References+ View more
- Seino Y, Tomita Y, Takano T, Hayakawa H. Early identification of cardiac events with serum troponin T in patients with unstable angina. Lancet 1993; 342: 1236-37
- Seino Y, Tomita Y, Hoshino K, Setsuta K, Takano T. Pathophysiological analysis of serum troponin T release kinetics in evolving ischemic myocardial injury. Jpn Circ J 1996; 60: 265-76
- Seino Y, Ogata K, Takano T, et al. Use of a whole blood rapid panel test for heart-type fatty acid-binding protein in patients with acute chest pain: Comparison with rapid troponin T and myoglobin test. Am J Med 2003; 15: 185-90
- Setsuta K, Seino Y, Takahashi N, et al. Clinical significance of elevated levels of cardiac Troponin T in patients with chronic heart failure. Am J Cardiol 1999; 84: 608-11
- Seino Y, Ogawa A, Yamashita T, et al. Application of NT-proBNP and BNP measurements in cardiac care: a more discerning marker for the detection and elevation of heart failure. Eur J Heart Fail 2004; 6: 295-300
- Thygessen K, et al. Universal definition of myocardial infarction. Eur Heart L 2007; 28: 2525-38
- Ogawa A, Seino Y, Ogata T, et al. Differences in elevation of NT-proBNP and conventional cardiac markers between patients with ST elevation and non-ST elevation acute coronary syndrome. Circ J 2006; 70: 1372-78
- Lindahl B, et al. Serial analyses of NT-proBNP in patients with non-ST-segment elevation acute coronary syndromes: a Fragmin and fast Revascularization during In Stability in Coronary artery disease (FRISC)-II substudy. J Am Coll Cardiol 2005; 45: 533-41
- Heeschen C, et al. N-terminal pro-BNP levels for dynamic risk stratification of patients with acute coronary syndromes. Circulation 2004; 110: 3206-12
- Setsuta K, Seino Y, et al. Clinical significance of elevated levels of cardiac troponin T in patients with chronic heart failure. Am J Cardiol 1999; 148: 141-49
- Setsuta K, Seino Y, et al. Use of cytosolic and myofibril markers in the detection of ongoing myocardial damage in patients with chronic heart failure. Am J Med 2002; 113: 717-22
References
- Seino Y, Tomita Y, Takano T, Hayakawa H. Early identification of cardiac events with serum troponin T in patients with unstable angina. Lancet 1993; 342: 1236-37
- Seino Y, Tomita Y, Hoshino K, Setsuta K, Takano T. Pathophysiological analysis of serum troponin T release kinetics in evolving ischemic myocardial injury. Jpn Circ J 1996; 60: 265-76
- Seino Y, Ogata K, Takano T, et al. Use of a whole blood rapid panel test for heart-type fatty acid-binding protein in patients with acute chest pain: Comparison with rapid troponin T and myoglobin test. Am J Med 2003; 15: 185-90
- Setsuta K, Seino Y, Takahashi N, et al. Clinical significance of elevated levels of cardiac Troponin T in patients with chronic heart failure. Am J Cardiol 1999; 84: 608-11
- Seino Y, Ogawa A, Yamashita T, et al. Application of NT-proBNP and BNP measurements in cardiac care: a more discerning marker for the detection and elevation of heart failure. Eur J Heart Fail 2004; 6: 295-300
- Thygessen K, et al. Universal definition of myocardial infarction. Eur Heart L 2007; 28: 2525-38
- Ogawa A, Seino Y, Ogata T, et al. Differences in elevation of NT-proBNP and conventional cardiac markers between patients with ST elevation and non-ST elevation acute coronary syndrome. Circ J 2006; 70: 1372-78
- Lindahl B, et al. Serial analyses of NT-proBNP in patients with non-ST-segment elevation acute coronary syndromes: a Fragmin and fast Revascularization during In Stability in Coronary artery disease (FRISC)-II substudy. J Am Coll Cardiol 2005; 45: 533-41
- Heeschen C, et al. N-terminal pro-BNP levels for dynamic risk stratification of patients with acute coronary syndromes. Circulation 2004; 110: 3206-12
- Setsuta K, Seino Y, et al. Clinical significance of elevated levels of cardiac troponin T in patients with chronic heart failure. Am J Cardiol 1999; 148: 141-49
- Setsuta K, Seino Y, et al. Use of cytosolic and myofibril markers in the detection of ongoing myocardial damage in patients with chronic heart failure. Am J Med 2002; 113: 717-22
May contain information that is not supported by performance and intended use claims of Radiometer's products. See also Legal info.


Acute care testing handbook
Get the acute care testing handbook
Your practical guide to critical parameters in acute care testing.
Download now
Scientific webinars
Check out the list of webinars
Radiometer and acutecaretesting.org present free educational webinars on topics surrounding acute care testing presented by international experts.
Go to webinars