Printed from acutecaretesting.org
April 2013
POCT of NT-proBNP in patients with renal disease





NT-PRO BNP IN DIALYSIS PATIENTS
Point of care (POC) testing has become an important part of nephrological care. Dialysis centers require POC testing of potassium, sodium, calcium and hematocrit levels, as well as rapid determination of acid-base status.
In cases of acute renal failure, POC is indispensable in deciding the need for dialysis, but is also essential in the management of patients on regular dialysis. In our dialysis center, we perform POC testing on each patient at least once per week.
Many of our patients suffer from diabetes, which requires knowledge of blood glucose levels before each dialysis. In addition, the use of anticoagulants during extravascular circulation requires POC monitoring of coagulation parameters.
Most dialysis patients suffer from a high level of co-morbidity.
Apart from diabetes, they often suffer from cardiovascular disease so that dialysis must not only restore blood electrolytes to normal but also remove excess water. POC testing may also help to identify hyperhydration, a diagnosis that is often difficult to make.
The main way of detecting hyperhydration is by an increase in body weight but this may be misleading, because weight loss or gain may be due to other causes.
An increase in blood pressure may also provide a clue, but many dialysis suffer from hypertension and arteriosclerosis or chronic heart failure so that raised blood pressure may not indicate hyperhydration while low blood pressure may appear with volume overload in patients with heart failure.
To achieve a good quality of dialysis, decisions about the dialysis prescription must be made beforehand or during the first 30 minutes of treatment, as the efficiency of dialysis decreases over time.
In patients with obesity - common among dialysis patients – a small percentage change in body weight may signal a large change in blood volume. Measurements of body impedance or ultrasound are too time-consuming to be performed before routine dialysis.
The same applies to radiology investigations such as a chest X-ray.
The high level of co-morbidity of our patients and the numerous obstacles that exist to accurately determining the amount of surplus fluid mean that complications are common, both during and after dialysis and in the inter-dialysis interval.
POC testing enables us to recognize and treat serious complications that may occur at any time such as arrhythmia, bleeding, and myocardial infarction and thromboembolism.
This means that in addition to conventional surveillance procedures such as continuous blood pressure measurement, oximetry and ECG monitoring, measurement of troponin, D-dimers and PTT/ACT must be available during dialysis.
Inflammation is a further serious problem often encountered by nephrologists. Dialysis patients require repeated vascular access by intravenous line or fistula, both of which are prone to infection.
The risk of infection is also increased by uremia-associated immunodeficiency. The main POC parameter used to detect infection is C-reactive protein (CRP).
Dialysis and hemodiafiltration remove n-terminal-pro-brain-type natriuretic peptide (NT-pro-BNP) from the circulation and change fluid volume. Nevertheless, Bargnoux and others were able to show that circulating BNP levels correlate with echocardiographic measurements such as the left ventricular mass index (1).
The addition of BNP to bio-impedance measurement may improve clinical and prognostic stratification of patients, as has already been shown for chronic systolic heart failure (2).
Recently, Bargnoux and colleagues showed that a combined index of troponin I, CRP and NT-pro-BNP improved estimation of risk of early cardiovascular mortality in hemodialysis patients (3).
The U.S. National Institutes of Health Registry of Clinical Studies (www.clinical.trials.gov) currently lists 30 studies of NT-pro-BNP measurement in renal disease (4). One of these is designed to investigate the correlation between NT-pro-BNP and other methods for regulating ultrafiltration in hemodialysis patients with fluid overload (5).
The combination of these diagnostic tools has been shown to reliably identify patients with a poor prognosis in other settings (6).
One Polish study found that “while there was only a moderate correlation between the NT-pro BNP level and hydration status, NT-pro-BNP was elevated in patients with intensive catabolism, severe anemia, higher mean arterial pressure and longer total duration of hemodialysis” (7).
This also applies to peritoneal dialysis, where NT-proBNP levels correlate with the degree of anemia, water balance, hyponatremia, and hypoalbuminemia.(8)
Anemia, electrolytes and albumin levels are already routinely monitored in all dialysis patients. NT-pro-BNP should now be added to this panel.
This test identifies additional risks and is particularly useful in patients with unclear symptoms in whom it may indicate which further diagnostic measures are required.
High NT-pro-BNP levels not only indicate increased morbidity, but have also been associated with increased mortality within two years of follow-up in stable out-patient hemodialysis patients with a best cut-off value of 18,611 pg/mL (9).
NT-PRO-BNP IN RENAL PATIENTS NOT ON DIALYSIS
Of course, nephrologists not only care for patients on dialysis but also for patients who have received a kidney transplant, patients with elevated blood pressure, and patients with chronic kidney disease in stages I to IV who do not (yet) require dialysis.Hypertensive patients referred to the specialist nephrologist are usually those whose blood pressure is poorly-controlled despite multiple antihypertensive medications, or those with other endocrine conditions or chronic kidney disease.
Many of these patients have serious vascular conditions. The figure shows that NT-pro BNP is elevated in renal insufficiency, is not related to GFR, and that changes in NT-pro-BNP provides information that would be missed by only monitoring the GFR, in particular information that would help to distinguish between sodium and volume overload.
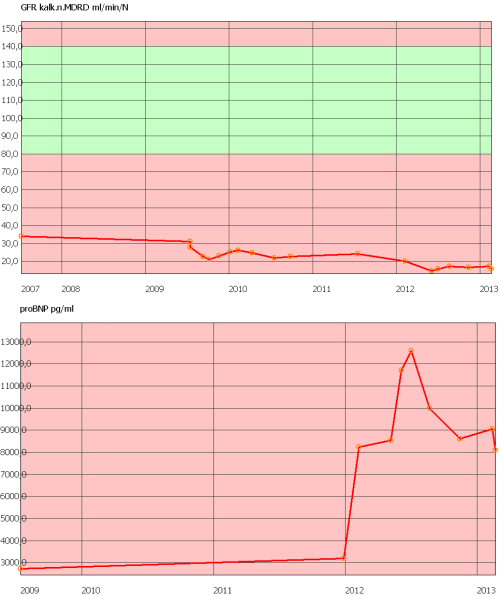
Figure: Glomerular filtration rate (upper panel) and level of of NT-pro BNP in patients with end-stage renal disease. Glomerular filtration rate (upper panel) and level of NT-pro BNP in a patient with advanced kidney disease. GFR declines slowly but continously. A rapid increase in NT-pro-BNP occurs when the clinical condition worsens.
Renal transplant recipients may develop acute graft failure even after a long stable period. Such cases may present as volume retention, the detection of which is improved by NT-pro-BNP measurement.
In patients with anemia of chronic disease, the degree of heart failure and vascular risk must be known to permit safe administration of erythropoietin, which also mandates measurement of NT-pro-BNP.
Patients with combined heart and renal failure are at high risk of death and must be treated with great care and urgency. This also applies to patients with other forms of cardio-renal syndrome.
Measurement of NT-pro-BNP forms an important part of this treatment and levels correlate with urine albumin excretion in patients with acute heart failure (10).
Diabetic nephropathy is not only one of the most common causes of renal failure, but also one of the most serious as it often causes a rapid decline in renal failure function with arrival at a “point of no return” at which dialysis becomes inevitable.
Since baseline NT-pro-BNP levels independently predict the annual rate of decline in the GFR, monitoring these is an important part of managing diabetic nephropathy.(11)
POC measurement of NT-pro-BNP is a new and important diagnostic tool that will improve treatment of renal patients, increasing safety and diagnostic accuracy while reducing the time required to determine appropriate therapy.
NT-pro-BNP is especially valuable in the context of the other tests already available to the nephrologist, where its addition will improve diagnostic and therapeutic accuracy.
The Cardiovascular Risk Reduction with Early Anaemia Treatment by Epoetin Beta (CREATE) study was a randomized multi-center study designed to explore the benefits of anemia correction in reducing cardiovascular risk in patients with chronic kidney disease.
In a sub-study of CREATE, NT-pro BNP-values above 400 pg/mL predicted the need for dialysis independently of hemoglobin levels (12).
Renal dysfunction increases the concentrations of both BNP and NT-proBNP (13); for this reason sequential measurements are superior to single measurements in patients with renal disease. Conversely, the finding of an increased NT-pro-BNP level may signal the possible presence of renal disease.
Neutrophil gelatin-associated lipocalin (NGAL) is a small protein that was originally found in neutrophil granules, but which is also present in the epithelium lining the loop of Henle and the glomerular collecting ducts.
Levels of NGAL in urine increase within two hours of renal ischemia. For this reason urinary NGAL is a useful addition to serum NT-pro-BNP in predicting renal dysfunction in patients with heart failure (14), a situation with which nephrologists are often confronted in the intensive care setting.
Another diagnostic tool for assessing prognosis in patients with pre-dialysis chronic kidney disease is the level of BNP in plasma (15). I believe the same may also be true for NT-pro-BNP as renal clearance does not vary significantly between the two brain-type natriuretic peptides (16, 17), although this view is not shared by Yasuda (15).
Contrary to claims that BNP and NT-ProBNP lose their predictive value in patients with renal dysfunction (15), both have been accurate in assessing prognosis in outpatients with heart failure and reduced GFR (18)
In acute pulmonary embolism, NT-pro-BNP is a good indicator of right ventricular volume and function (19). However, because NT-pro-BNP levels are increased in renal failure the additional measurement of D-dimer concentrations is required in patients with thromboembolic disease.
Although the specificity of the natriuretic peptides and the troponins is decreased in renal failure, the measurement of a combination of both is reliable.
NT-pro-BNP is important not only in dialysis patients but also in pre-dialysis individuals. As Desai and colleagues have noted, “these cardiac-derived biomarkers (TnT and NT-pro-BNP) enhance prediction of end-stage renal disease (ESRD) beyond established risk factors.
Measurement of troponin T and NT-pro-BNP may improve the identification of patients with CKD who are likely to require renal replacement therapy, supporting a link between cardiac injury and the development of ESRD” (20).
It is sometimes difficult to decide the exact date for commencing long-term dialysis in patients with ESRD. Such cases include elderly patients in whom the primary goal of dialysis is not to extend life but to allow the patient a degree of self-sufficiency.
From personal experience, I recommend measuring NT-Pro-BNP in such cases as an aid to estimating the risk of serious complications and thereby loss of autonomy if dialysis is not initiated. In this setting, the ratio of NT-pro-BNP to GFR has proved helpful.
In conclusion, NT-pro-BNP has become an indispensable diagnostic tool in nephrology. Accurate POC testing for NT-pro-BNP should be available in all dialysis and large nephrology centers.
|
Clinical condition |
Additional point-of-care parameter |
| Sepsis | CRP |
| Imminent need for dialysis | GFR |
| Myocardial infarction/myocardial ischemia | Troponin-T |
| Embolism | D-Dimer |
| Volume overload | Sodium |
| Calculation of required dosage of erythropoietin | Hemoglobin |
Table: Conditions in which additional point-of-care parameters should be measured in addition to NT-pro-BNP in patients with chronic kidney disease.
ACKNOWLEDGMENT
The author is very thankful to Professor Paul Cullen, Managing Director of Medizinisches Labor in Muenster, Germany, for his expert review and proofreading of this article.
References+ View more
- Bargnoux A-S, Klouche K, Fareh J, Barazer I, Villard-Saussine S, Dupuy A-M, et al. Prohormone brain natriuretic peptide (proBNP), BNP and N-terminal-proBNP circulating levels in chronic hemodialysis patients. Correlation with ventricular function, fluid removal and effect of hemodiafiltration. Clin Chem Lab Med. 2008;46(7):1019–24.
- Malfatto G, Corticelli A, Villani A, Giglio A, Rosa Della F, Branzi G, et al. Transthoracic bioimpedance and brain natriuretic Peptide assessment for prognostic stratification of outpatients with chronic systolic heart failure. Clin Cardiol. 2013 Feb;36(2):103–9.
- Bargnoux A-S, Morena M, Jaussent I, Maurice F, Chalabi L, Leray-Moragues H, et al. A combined index of cardiac biomarkers as a risk factor for early cardiovascular mortality in hemodialysis patients. Clin Chem Lab Med. 2013 Feb 11;:1–10.
- clinicaltrials.gov [Internet]. [cited 2013 Feb 24]. Available from: http://www.clinicaltrials.gov
- Hecking M, Antlanger M, Winnicki W, Reiter T, Werzowa J, Haidinger M, et al. Blood volume-monitored regulation of ultrafiltration in fluid-overloaded hemodialysis patients: study protocol for a randomized controlled trial. Trials. 2012;13:79.
- Bielecka-Dabrowa A, Haehling von S, Aronow WS, Ahmed MI, Rysz J, Banach M. Heart failure biomarkers in patients with dilated cardiomyopathy. Int J Cardiol. Elsevier Ireland Ltd; 2013 Feb 13;:1–7.
- Bednarek-Skublewska A, Zaluska W, Ksiazek A. The relationship between serum level of N-terminal pro-B-type natriuretic peptide and nutritional status, and inflammation in chronic hemodialysis patients. Clin. Nephrol. 2010 Jan;73(1):14–20.
- Adachi Y, Nishio A. N-terminal pro-brain natriuretic peptide in prevalent peritoneal dialysis patients. Adv Perit Dial. 2008;24:75–8.
- Artunc F, Mueller C, Breidthardt T, Twerenbold R, Rettig I, Usta E, et al. Comparison of the Diagnostic Performance of Three Natriuretic Peptides in Hemodialysis Patients: Which is the Appropriate Biomarker?. Kidney Blood Press. Res. 2012 Oct 30;36(1):172–81.
- Koyama S, Sato Y, Tanada Y, Fujiwara H, Takatsu Y. Early Evolution and Correlates of Urine Albumin Excretion in Patients Presenting with Acutely Decompensated Heart Failure. Circ Heart Fail. 2013 Feb 8.
- Seki N, Nishimura M, Matsumoto T, Fukazawa M, Kenmochi T. Relationship between BNP level and renal function in diabetic nephropathy with microalbuminuria. J. Diabetes Complicat. 2013 Jan;27(1):92–7.
- USE OF BNP-TYPE PEPTIDES FOR PREDICTING DIALYSIS NEED. US Patent Office; 2008.
- Srisawasdi P, Vanavanan S, Charoenpanichkit C, Kroll MH. The Effect of Renal Dysfunction on BNP, NT-proBNP, and Their Ratio. American Journal of Clinical Pathology. 2010 Jan 1;133(1):14–23.
- Palazzuoli A, Beltrami M, Pellegrini M, Nuti R. Natriuretic peptides and NGAL in heart failure: does a link exist? Clin. Chim. Acta. 2012 Nov 20;413(23-24):1832–8.
- Yasuda K, Kimura T, Sasaki K, Obi Y, Iio K, Yamato M, et al. Plasma B-type natriuretic peptide level predicts kidney prognosis in patients with predialysis chronic kidney disease. Nephrol Dial Transplant. 2012 Oct;27(10):3885–91.
- Palmer SC, Richards AM. Does Renal Clearance Differ Between the B-Type Natriuretic Peptides (BNP Versus NT-proBNP). JAC. American College of Cardiology Foundation; 2009 Mar 10;53(10):891–2.
- van Kimmenade RRJ, Januzzi JL, Bakker JA, Houben AJ, Rennenberg R, Kroon AA, et al. Renal Clearance of B-Type Natriuretic Peptide and Amino Terminal Pro-B-Type Natriuretic Peptide. JAC. American College of Cardiology Foundation; 2009 Mar 10;53(10):884–90.
- Waldum B, Stubnova V, Westheim AS, Omland T, Grundtvig M, Os I. Prognostic utility of B-type natriuretic peptides in patients with heart failure and renal dysfunction. Clinical Kidney Journal. 2013 Jan 30;6(1):55–62.
- Pasha SM, Klok FA, van der Bijl N, de Roos A, Kroft LJM, Huisman MV. NT-pro-BNP levels in patients with acute pulmonary embolism are correlated to right but not left ventricular volume and function. Thromb. Haemost. 2012 Aug;108(2):367–72.
- Desai AS, Toto R, Jarolim P, Uno H, Eckardt K-U, Kewalramani R, et al. Association between cardiac biomarkers and the development of ESRD in patients with type 2 diabetes mellitus, anemia, and CKD. Am J Kidney Dis. 2011 Nov;58(5):717–28.
References
- Bargnoux A-S, Klouche K, Fareh J, Barazer I, Villard-Saussine S, Dupuy A-M, et al. Prohormone brain natriuretic peptide (proBNP), BNP and N-terminal-proBNP circulating levels in chronic hemodialysis patients. Correlation with ventricular function, fluid removal and effect of hemodiafiltration. Clin Chem Lab Med. 2008;46(7):1019–24.
- Malfatto G, Corticelli A, Villani A, Giglio A, Rosa Della F, Branzi G, et al. Transthoracic bioimpedance and brain natriuretic Peptide assessment for prognostic stratification of outpatients with chronic systolic heart failure. Clin Cardiol. 2013 Feb;36(2):103–9.
- Bargnoux A-S, Morena M, Jaussent I, Maurice F, Chalabi L, Leray-Moragues H, et al. A combined index of cardiac biomarkers as a risk factor for early cardiovascular mortality in hemodialysis patients. Clin Chem Lab Med. 2013 Feb 11;:1–10.
- clinicaltrials.gov [Internet]. [cited 2013 Feb 24]. Available from: http://www.clinicaltrials.gov
- Hecking M, Antlanger M, Winnicki W, Reiter T, Werzowa J, Haidinger M, et al. Blood volume-monitored regulation of ultrafiltration in fluid-overloaded hemodialysis patients: study protocol for a randomized controlled trial. Trials. 2012;13:79.
- Bielecka-Dabrowa A, Haehling von S, Aronow WS, Ahmed MI, Rysz J, Banach M. Heart failure biomarkers in patients with dilated cardiomyopathy. Int J Cardiol. Elsevier Ireland Ltd; 2013 Feb 13;:1–7.
- Bednarek-Skublewska A, Zaluska W, Ksiazek A. The relationship between serum level of N-terminal pro-B-type natriuretic peptide and nutritional status, and inflammation in chronic hemodialysis patients. Clin. Nephrol. 2010 Jan;73(1):14–20.
- Adachi Y, Nishio A. N-terminal pro-brain natriuretic peptide in prevalent peritoneal dialysis patients. Adv Perit Dial. 2008;24:75–8.
- Artunc F, Mueller C, Breidthardt T, Twerenbold R, Rettig I, Usta E, et al. Comparison of the Diagnostic Performance of Three Natriuretic Peptides in Hemodialysis Patients: Which is the Appropriate Biomarker?. Kidney Blood Press. Res. 2012 Oct 30;36(1):172–81.
- Koyama S, Sato Y, Tanada Y, Fujiwara H, Takatsu Y. Early Evolution and Correlates of Urine Albumin Excretion in Patients Presenting with Acutely Decompensated Heart Failure. Circ Heart Fail. 2013 Feb 8.
- Seki N, Nishimura M, Matsumoto T, Fukazawa M, Kenmochi T. Relationship between BNP level and renal function in diabetic nephropathy with microalbuminuria. J. Diabetes Complicat. 2013 Jan;27(1):92–7.
- USE OF BNP-TYPE PEPTIDES FOR PREDICTING DIALYSIS NEED. US Patent Office; 2008.
- Srisawasdi P, Vanavanan S, Charoenpanichkit C, Kroll MH. The Effect of Renal Dysfunction on BNP, NT-proBNP, and Their Ratio. American Journal of Clinical Pathology. 2010 Jan 1;133(1):14–23.
- Palazzuoli A, Beltrami M, Pellegrini M, Nuti R. Natriuretic peptides and NGAL in heart failure: does a link exist? Clin. Chim. Acta. 2012 Nov 20;413(23-24):1832–8.
- Yasuda K, Kimura T, Sasaki K, Obi Y, Iio K, Yamato M, et al. Plasma B-type natriuretic peptide level predicts kidney prognosis in patients with predialysis chronic kidney disease. Nephrol Dial Transplant. 2012 Oct;27(10):3885–91.
- Palmer SC, Richards AM. Does Renal Clearance Differ Between the B-Type Natriuretic Peptides (BNP Versus NT-proBNP). JAC. American College of Cardiology Foundation; 2009 Mar 10;53(10):891–2.
- van Kimmenade RRJ, Januzzi JL, Bakker JA, Houben AJ, Rennenberg R, Kroon AA, et al. Renal Clearance of B-Type Natriuretic Peptide and Amino Terminal Pro-B-Type Natriuretic Peptide. JAC. American College of Cardiology Foundation; 2009 Mar 10;53(10):884–90.
- Waldum B, Stubnova V, Westheim AS, Omland T, Grundtvig M, Os I. Prognostic utility of B-type natriuretic peptides in patients with heart failure and renal dysfunction. Clinical Kidney Journal. 2013 Jan 30;6(1):55–62.
- Pasha SM, Klok FA, van der Bijl N, de Roos A, Kroft LJM, Huisman MV. NT-pro-BNP levels in patients with acute pulmonary embolism are correlated to right but not left ventricular volume and function. Thromb. Haemost. 2012 Aug;108(2):367–72.
- Desai AS, Toto R, Jarolim P, Uno H, Eckardt K-U, Kewalramani R, et al. Association between cardiac biomarkers and the development of ESRD in patients with type 2 diabetes mellitus, anemia, and CKD. Am J Kidney Dis. 2011 Nov;58(5):717–28.
May contain information that is not supported by performance and intended use claims of Radiometer's products. See also Legal info.


Acute care testing handbook
Get the acute care testing handbook
Your practical guide to critical parameters in acute care testing.
Download now
Scientific webinars
Check out the list of webinars
Radiometer and acutecaretesting.org present free educational webinars on topics surrounding acute care testing presented by international experts.
Go to webinars