Printed from acutecaretesting.org
January 2007
Sleep like a baby?




acutecaretesting.org: When did you implement PSG in the NICU at Halmstad?
Dan Andersson: We have had our present PSG setup for one year, but have had the technology and specialty since 1990. With regard to neonatal patients and children up to 10 kg, we cover the entire region of southern Sweden. There are other sleep laboratories for larger children in Gothenburg and Lund, and one in Stockholm that covers the north of Sweden.
Why the specialty is here in Halmstad NICU? Because I brought it with me from a previous position at the University Hospital MAS, Sweden, where I started my research in respiratory physiology and sleep disorders in 1985.
Our setup in Halmstad is one of the most comprehensive ones in Scandinavia. Similar setups are used in the Great Ormond Street Hospital in London, England, and in other sleep laboratories in Europe. The PSG setup is built onto a roller stand, which means that we don’t need to have a dedicated bed site in the unit.
acutecaretesting.org: Please describe what PSG is?
PSG is a diagnostic test in which a number of physiologic variables are measured and recorded during sleep. By analyzing the data it is possible to diagnose various conditions such as sleep apnea, epilepsy and cramps, snoring and ALTE (Apparent Life-Threatening Events). And just as important, to “dismiss” those patients who are not endangered by their breathing patterns.
The PSG setup may vary from one clinic to another. The data we include in our extended PSG setup include brain electrical activity (sleep stage), eye movement, arm movement, airflow, respiratory effort, cardiac rhythm, oxygen saturation and transcutaneous gases, i.e. pCO2 and pO2.
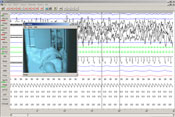
We also record sound, e.g. snoring, and an infrared image of the sleeping baby. All data are collected in a single file, which means that the interdependency of the signals is easily tracked.
acutecaretesting.org: Who are the patients?
Most of our patients are otherwise healthy babies, who have had one or more occasions of sleep apnea where they have been found not breathing in their sleep. The parents are afraid that their baby may die from sudden infant’s death syndrome (SIDS) and they come here for a diagnosis.
We are sometimes able to reconstruct the symptoms here in the NICU under safe conditions, by spraying a little water into the nose of the baby. The water causes apnea, the child's lips and skin turn bluish and finally the child draws a new breath.
The parents recognize the symptoms and are relieved to know that the condition is harmless and that their baby has a well-functioning arousal mechanism that will prompt it to take a breath when needed.
Some babies show signs of disease such as excessive obstructive apneas or neurological disease but most of the children don’t show any abnormality.
Other patients may already be cared for in our NICU for other reasons. Any baby who shows excessive symptoms of apnea that cannot be explained by natural causes will be monitored with PSG to determine the condition of the apnea.
The common PSG patient is a 4-kg neonate but also larger children, up to 10 kg, are monitored.
acutecaretesting.org: How do you prepare the patient for monitoring?
Camilla Cronqvist: It takes about an hour to attach all electrodes. After that, the child is exhausted and usually ready to go to sleep. I don’t  connect the cords to the monitor until the child is ready to be tugged into bed.
connect the cords to the monitor until the child is ready to be tugged into bed.
Most children dislike all the fiddling and preparations. It is not painful but annoying. As a consequence, when I train colleagues, I let them practice on a doll before they work with the patients.
The parent (most often the mother) will hold the child to comfort it and she often helps with the applications to speed up the process. It also helps alleviate the discomfort when we give a few drops of 30 % glucose solution on the tongue.
First, I attach the EEG electrodes and the eye movement electrodes and collect the cords in a ponytail of tube gauze.
After a little rest and feeding, the remaining sensors and bands are attached and the cords collected in a second ponytail to minimize the discomfort to the child.
The child is tired by now and may already be sleeping in the arms of the parent. All electrodes are connected to the PSG, the camera is turned on and I can retreat to the reception area where the signals can be followed on the monitor.
At least once an hour, I check the signals and note the status of the baby, e.g. sleeping, feeding or crying.
acutecaretesting.org: How do you evaluate the recordings?
Dan Andersson: I search for specific patterns in the signals. We have predefined several patterns in the software, which makes it easier to scroll through the data file. Patterns linked to tidal volume, obstructive apnea periods, etc.
I prefer to keep an objective eye to the evaluation so I usually don’t know the patient’s story in advance. When I have studied every event that the software identifies, I write a conclusion, which is sent to the referring doctor with a print of the data.
|
Evaluation of one night’s recordings may include 4-800 events and may take hours, even though I have everything digitally available on one screen. Years ago, when we had only paper prints of data, e.g. from tc gases and EKG electrodes, it was really time-consuming to identify patterns. The screen dump shows an example of recording as presented on the screen. |
acutecaretesting.org: What are the most common diagnoses from your evaluations?
The most common message we give to parents is that their baby is healthy and suffers no sleep disorder. When we find that the gases fluctuate with respiratory rhythm and that the child has a satisfying arousal mechanism and starts breathing spontaneously, the diagnosis may be an uncomplicated neonatal sleep apnea and the child can go home with the parents.
In some infants we find abnormalities such as excessive obstructive apneas or hypoventilation. Also prolonged central apneas and neurological diseases, such as cramps, can be diagnosed with this setup.
acutecaretesting.org: What advantage do you see from the combination of saturation and transcutaneous gases?
Dan Andersson: I consider them part of the complete respiratory picture – they supplement each other. We have set the tc temperature at 42 °C and, consequently, we get fairly low tcpO2 values.
When I compare all three signals, I can use the patterns to recognize the real events and rule out electrode drift or movement artefacts. Say that tcpCO2 increases while tcpCO2 and SpO2 decrease – the pattern is a hypoventilatory match. On the other hand, if only tcpCO2 increased and the other values were normal, it was likely to be a system drift.
acutecaretesting.org: How do you see the future for PSG at Halmstad?
With our present patient population, we will maintain our specialty here at Halmstad. The neonatal PSG population is very small compared with the large adult population who suffers from sleep disorders – undiagnosed, I might add. The consequences of sleep disorders are many – regardless of the patient being a child or an adult.
I believe we will see more PSG research in our unit. The access to single-file data of high quality makes evaluation of studies easier. We see more and more indications, also in the young population.
INTERVIEWEES
Nurse Camilla Cronqvist
Clinical engineer Fredrik Kaestner
Neonatologist Dan Andersson
CONTACT
Dan Andersson
Head of department of Paediatrics,
Halmstad County Hospital
Sweden
INTERVIEWER
Gitte Juel
Radiometer Medical ApS
Åkandevej 21
2700 Brønshøj
Denmark


Acute care testing handbook
Get the acute care testing handbook
Your practical guide to critical parameters in acute care testing.
Download now
Related webinar
Transcutaneous monitoring in the sleep center - Is this really necessary?
Webinar presented by Julie DeWitte, RPSGT, RST, RCP - Asst. Administrator, Sleep Disorders Center Kaiser Permanente Fontana Medical Center, Fontana, CA Watch the webinar
Related webinar
Evolution of blood gas testing Part 1
Presented by Ellis Jacobs, PhD, Assoc. Professor of Pathology, NYU School of Medicine.
Watch the webinar